Internal Medicine Oklahoma State University Medical Center Tulsa, Oklahoma, United States
Clinical Scenario or Case: The patient is a 45-year-old male with a history of chronic kidney disease stage 3b, type-1 diabetes mellitus, peripheral arterial disease, and hypothyroidism, who presented to our facility from another facility for worsening acute kidney injury (AKI) following treatment for diabetic ketoacidosis.
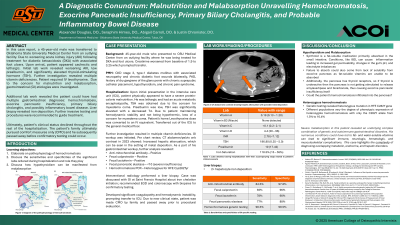
On arrival, the patient appeared cachectic and lethargic. Lab work revealed worsening creatinine, low prealbumin, and an elevated TSH. Vitamin studies revealed multiple deficiencies. Nephrology started hemodialysis. Vitamin supplementation and intravenous levothyroxine were initiated. Due to his malnutrition and malabsorption, gastrointestinal etiologies were investigated. Prior imaging showed hepatic metal deposition and iron studies showed increased iron saturation, thus prompting hemochromatosis genetic testing, which identified a heterozygous C282Y mutation. Additional findings included severe pancreatic insufficiency, positive fecal calprotectin and lactoferrin, positive anti-mitochondrial antibody, and a liver biopsy with 2+ hepatocyte iron deposition. Gastroenterology recommended esophagogastroduodenoscopy and colonoscopy with biopsies to guide further management; however, the patient developed coagulopathy and hemodynamic instability. Comfort measures were pursued, and he subsequently passed away. This case highlights the complexity of diagnosing overlapping metabolic, endocrine, and hepatic disorders.
Evidence/Literature Review: Malabsorption has a broad etiology, including inadequate intake and structural or functional gastrointestinal (GI) disorders. Resulting deficiencies in fat- and water-soluble vitamins can lead to significant immune, neurologic, hematologic, and musculoskeletal complications. The coexistence of multiple deficiencies should prompt investigation for underlying GI pathology.
Unique Aspects of Case: Severe malabsorption in this patient revealed an underlying complex combination of genetic and autoimmune gastrointestinal disorders. Hemochromatosis, combined with pancreatic infiltration, likely caused exocrine insufficiency and fat-soluble vitamin deficiencies, while concurrent water-soluble deficiencies suggested additional small bowel pathology.
Recommendations/Conclusions: Malabsorption is a common presentation, often due to poor dietary habits. However, when a patient presents this severe, it should raise the suspicion for an underlying GI disorder. Earlier identification of the source of malabsorption can lead to improved supplementation and reduced morbidity/mortality.

 photo")