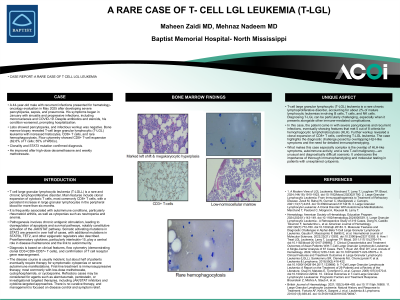
Clinical Scenario or Case: A 44-year-old male with recurrent infections presented for hematology-oncology evaluation in May 2025 after developing severe pancytopenia, sepsis, and pneumonia. His symptoms began in January with sinusitis and progressive infections, including mononucleosis and COVID-19. Despite antibiotics and steroids, his condition worsened, prompting hospitalization. Labs showed pancytopenia, and infectious workup was negative. Bone marrow biopsy revealed T-cell large granular lymphocytic (T-LGL) leukemia with increased histiocytes, CD8+ T cells, and rare hemophagocytosis. Flow cytometry showed CD8+ T-cell expansion (62.6% of T cells; 55% of WBCs). Clonality and STAT3 mutation confirmed diagnosis. He improved after high-dose dexamethasone and methotrexate.
Evidence/Literature Review: T-cell large granular lymphocytic leukemia (T-LGLL) is a rare, indolent lymphoproliferative disorder marked by clonal expansion of cytotoxic T cells. It is frequently associated with pancytopenia and autoimmune conditions. Though typically seen in older adults, younger patients may also be affected, often presenting atypically. Diagnosis requires persistent lymphocytosis, T-cell clonality, and exclusion of other causes. Somatic STAT3 mutations support the diagnosis. Treatment is reserved for symptomatic cytopenias or autoimmune complications, with methotrexate as first-line therapy and other immunosuppressants or targeted agents used for refractory cases.
Unique Aspects of Case: It is a rare chronic lymphoproliferative disorder, making up about 2% of mature lymphocytic leukemias. Diagnosing it can be difficult, especially with overlapping immune complications. This patient presented with pancytopenia and recurrent infections, meeting 5 of 8 HLH criteria. Clonal CD8+ T-cell expansion confirmed T-LGL. The case highlights the diagnostic challenge posed by overlapping HLH-like symptoms and the need for detailed immunophenotyping.
Recommendations/Conclusions: T-cell large granular lymphocytic leukemia (T-LGLL) is a chronic lymphoproliferative disorder marked by clonal expansion of CD8+ T cells and persistent cytopenias. It is often associated with autoimmune diseases. Diagnosis involves flow cytometry and T-cell clonality testing. Treatment focuses on immunosuppression, with no curative options currently available.