Osteopathic Medical Student Lincoln Memorial University - DeBusk College of Osteopathic Medicine Knoxville, Tennessee, United States
Clinical Scenario or Case: A 25-year-old male presented to clinic with dysphagia and gastroesophageal reflux disease. One month prior, he was given a suspected diagnosis of eosinophilic esophagitis (EoE) after a hospital visit for food bolus. Physical exam was unremarkable aside from an underweight body mass index of 18.2. He was placed on Flovent therapy for 4 weeks with improvement of chest tightness from daily to once weekly. He proceeded with esophagogastroduodenoscopy (EGD) 12 weeks later to assess therapy effectiveness.
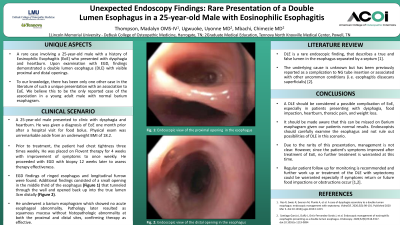
EGD revealed a non-bleeding diverticulum with a small opening and no stigmata of recent bleeding found in the middle third of the esophagus. This tunneled through the esophagus wall and reopened into the true lumen 3cm distally.
Evidence/Literature Review: Esophageal Diverticulum (ED) is a rare phenomenon of outpouching of the esophageal mucosa affecting less than 1% of the population. Most commonly these are asymptomatic and present in people over the age of 50, especially over the age of 70.
Unique Aspects of Case: To our knowledge, there has never been a report of such a unique diverticulum with two connections in the mid-esophagus, especially in a young adult male in the context of EoE. The patients age, symptoms, and rare ED anatomy make this case presentation unique and educational.
Recommendations/Conclusions: Endoscopists should carefully examine the esophagus for diverticulum especially in patients with persistent symptoms in the setting of pathologic remission of EoE. In cases when an ED is found, a distal opening should be carefully sought for during the EGD as passing the scope blindly could lead to perforation. Further workup with Chest CT and Barium Swallow should be conducted to rule out mediastinal causes such as malignancy of the thorax and development of esophagobronchial or tracheoesophageal fistulas.