Internal Medicine Rutgers-Jersey City Medical Center Jersey City, New Jersey, United States
Clinical Scenario or Case: A 25-year-old African American male with no known history presented with fever, fatigue, night sweats, joint pain, anorexia, and pleuritic chest pain. Examination revealed bilateral sub-centimeter breast nodules. Labs showed WBC 3.5 K/µL, hemoglobin 9.4 g/dL, normal renal function, elevated inflammatory markers, hypergammaglobulinemia, and hypoalbuminemia. Infectious workup was negative; EBV-IgG was positive. Autoimmune testing revealed ANA 1:320, dsDNA 28 IU/mL, low complements, RF 38, and elevated SSA and ribosomal-P antibodies.
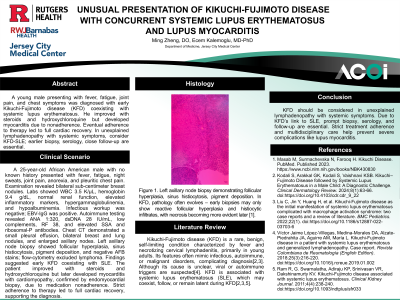
Chest CT demonstrated a small pleural effusion, bilateral breast and lung nodules, and enlarged axillary nodes. Left axillary node biopsy showed follicular hyperplasia, sinus histiocytosis, pigment deposition, and negative AFB stains; flow-cytometry excluded lymphoma. Findings suggested early KFD coexisting with SLE.
The patient improved with steroids and hydroxychloroquine but later developed myocarditis with cardiomyopathy, confirmed by endomyocardial biopsy, due to nonadherence. Strict adherence to therapy led to full cardiac recovery, confirming the diagnosis.
Evidence/Literature Review: Kikuchi-Fujimoto disease (KFD) is a rare, benign, self-limiting condition characterized by fever and necrotizing cervical lymphadenitis, primarily in young adults. Its features often mimic infectious, autoimmune, or malignant disorders, complicating diagnosis[1,2]. Although its cause is unclear, viral or autoimmune triggers are suspected[3]. KFD is associated with systemic lupus erythematosus (SLE), which may coexist, follow, or remain latent during KFD[1,2,4].
Unique Aspects of Case: This case is unique due to the rare coexistence of KFD and SLE in an African American male, as KFD predominantly affects young Asian women. The presentation with bilateral breast nodules and multiple pulmonary nodules is highly atypical for both conditions, adding to the diagnostic complexity. Furthermore, the development of lupus myocarditis with cardiomyopathy is an uncommon but severe complication.
Recommendations/Conclusions: KFD should be considered in unexplained lymphadenopathy with systemic symptoms. Because of its link to SLE, prompt biopsy, serology, and follow-up are essential. Strict treatment adherence and multidisciplinary care help prevent severe complications like lupus myocarditis.