Clinical Scenario or Case: A nonbinary biological male over age 30 with a history of HIV (CD4 count unknown) and nephrotic kidney disease presented to the ED with acute-on-chronic right knee pain impairing ambulation. The patient was last seen in the ED 7 months ago for similar complaints, where an x-ray of the femur demonstrated patchy sclerotic changes at the superior femoral head with no evidence of subchondral collapse, characteristic of avascular necrosis (AVN). The patient underwent further MRI testing, showing AVN in multiple large joints. The patient will be following up with orthopedic surgery to discuss surgical treatment options.
Evidence/Literature Review: Avascular necrosis of the femoral head is one of the most debilitating musculoskeletal complications in HIV, caused by insufficient blood flow to the femoral subchondral bone. It is likely multifactorial in origin, related to corticosteroid use, antiretroviral therapy, coagulopathy, and endothelial dysfunction. If left untreated, AVN can progress to collapse of the femoral head and osteoarthritis.
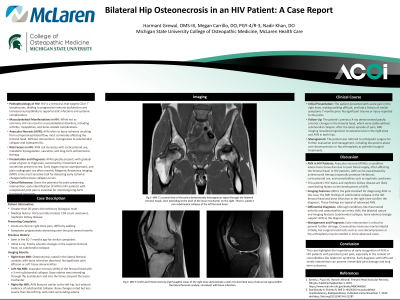
Unique Aspects of Case: The patient underwent MRI of the right knee, revealing osteonecrosis within the lateral femoral condyle. MRI of the left hip revealed AVN of the femoral head with evidence of subchondral collapse measuring up to 3 mm. Bony edema extended throughout the acetabulum and within the femur, extending beyond the level of the lesser trochanter. MRI of the right hip demonstrated similar findings to the left but without subchondral collapse.
Recommendations/Conclusions: This case highlights the importance of an early MRI screening for AVN in HIV patients with persistent joint pain. Early diagnosis and intervention can prevent irreversible joint damage and improve long-term function. Given the progressive and multifocal nature of AVN in this patient, early orthopedic referral is essential, especially in the setting of multiple risk factors. This case also underscores the need for ongoing surveillance in patients with overlapping systemic risk factors for osteonecrosis.