Internal Medicine Broward Health Medical Center Sunrise, Florida, United States
Clinical Scenario or Case: We present a case of a 42 year-old male with a past medical history of diabetes and IV drug use evaluated for fever, chills and shortness of breath. On admission, he was tachycardic and hypotensive. CT abdomen and pelvis showed findings representing multifocal embolic phenomenon with septic emboli. A CT brain showed no acute intracranial abnormality.
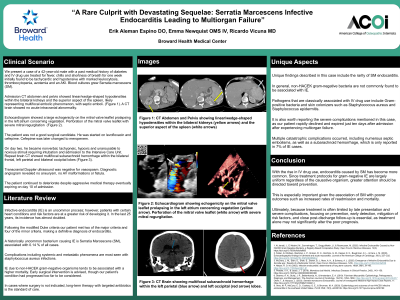
Blood cultures grew Serratia marcescens (SM). Echocardiogram showed evidence of vegetations. He was diagnosed with endocarditis and started on antibiotic therapy.
On day two he became nonverbal and unarousable to noxious stimuli. Repeat CT brain showed multifocal subarachnoid hemorrhage. He continued to deteriorate despite aggressive medical therapy and expired on day ten.
Evidence/Literature Review: Infective endocarditis (IE) is uncommon; however, patients with certain heart conditions and risk factors are at a greater risk of developing it. In the last 25 years, the incidence of IE has more than doubled.
Bacterial organisms are the most common causes of IE. Non-HACEK organisms are associated with around 2 % of cases. A historically uncommon bacterium is SM, causing around 0.14 % of all cases, and is associated with a higher mortality.
Unique Aspects of Case: Unique findings described in this case include the rareness of SM endocarditis, which has only been reported in 0.1 to 0.3 % of IE cases. The severe complications are also notable in this case, as our patient rapidly declined and expired just ten days after admission due to multiple catastrophic complications including numerous septic embolisms, as well as a subarachnoid hemorrhage, which is only reported in 7% of IE cases.
Recommendations/Conclusions: Since treatment protocols for gram negative IE are largely uniform regardless of the causative organism, greater attention should be directed toward prevention. This is especially important given the association of SM with poorer outcomes.