Internal Medicine Oklahoma State University Medical Center Tulsa, Oklahoma, United States
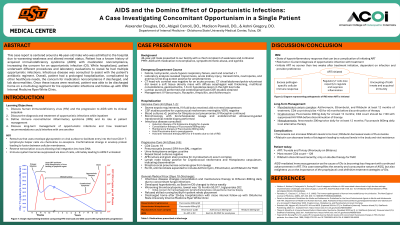
Clinical Scenario or Case: A 46 year-old male with a past medical history of acquired immunodeficiency syndrome (AIDS), mycobacterium avium complex (MAC), syphilis, and methamphetamine abuse presented with a chief complaint of weakness and altered mental status (AMS). In the emergency department, he was febrile, tachycardic, and hypoxic on room air. Laboratory studies revealed acute kidney injury, troponinosis, and transaminitis. Following a lumbar puncture, he was admitted to the intensive care unit for severe sepsis with altered mental status.
During hospitalization, the patient was diagnosed with multiple opportunistic infections (OIs) in the setting of profound immunosuppression, with a CD4 count of 19. Cerebrospinal fluid analysis confirmed cryptococcal meningitis. Additional studies revealed disseminated cryptococcus, disseminated histoplasmosis, persistent disseminated MAC. Following completion of intravenous therapy, infectious disease recommended the following discharge regimen: Antiretroviral therapy (ART) 4-6 weeks after antifungal treatment; fluconazole for consolidation and maintenance of cryptococcosis and histoplasmosis; azithromycin, rifampin, and ethambutol for MAC; and Bactrim-DS for Pneumocystis jirovecii prophylaxis. He continues to receive care through the OSU Internal Medicine HIV Clinic.
Evidence/Literature Review: In the context of AIDS-associated immunosuppression, opportunistic infections (OIs) are notably more frequent and severe. This case underscores the critical importance of early human immunodeficiency virus (HIV) diagnosis and intervention, while also highlighting the clinical complexity of initiating antiretroviral therapy in the setting of concurrent OIs due to the potential development of immune reconstitution inflammatory syndrome (IRIS).
Unique Aspects of Case: Not only was the patient diagnosed with cryptococcal meningitis, but he also had disseminated cryptococcus confirmed by lymph node biopsy. While having concomitant histoplasmosis, the guidelines have different anti-fungal recommendations, thus complicating treatment standards.
Recommendations/Conclusions: AIDS-mediated immunosuppression as the cause of OIs is becoming less frequent with continued advancements in ART. This case exemplifies the severity and consumptive nature of AIDS, but also enlightens us on the importance of the prophylactic and definitive treatment strategies of OIs.

 photo")