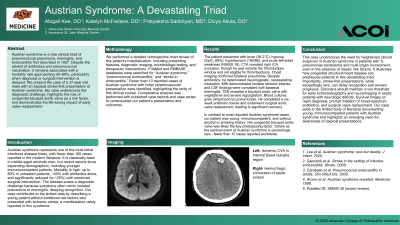
Clinical Scenario or Case: A 37-year-old male with a history of seizures presented with abrupt-onset left-sided weakness, fever, and respiratory distress. On exam, he was febrile (38.2°C), hypoxic (SpO₂ 89%), hypertensive (BP 190/86), and lethargic, with NIHSS of 18. Imaging revealed occlusion of the right internal carotid artery; he was outside the thrombolytic window and not a candidate for thrombectomy. Workup revealed bilateral pneumonia. He deteriorated neurologically and was intubated. Brain MRI indicated embolic strokes and probable purulent debris consistent with meningitis. TEE showed a bicuspid aortic valve with vegetations and moderate-to-severe regurgitation. Blood cultures grew Streptococcus pneumoniae, confirming the diagnosis of Austrian syndrome (pneumococcal meningitis, pneumonia, and endocarditis). The patient completed antibiotics, underwent successful aortic valve replacement, and is recovering well.
Evidence/Literature Review: Austrian syndrome is a rare, life-threatening triad first described by Robert Austrian in 1957. It typically affects middle-aged males and is associated with predisposing factors such as alcohol use, cigarette smoking, and immunocompromise. The syndrome has high morbidity and mortality, often requiring early diagnosis, IV antibiotics, and surgical intervention.
Unique Aspects of Case: This case highlights Austrian syndrome in a young adult without classic risk factors. The patient’s bicuspid aortic valve may have contributed to susceptibility. Presentation with large-vessel stroke, rather than meningitic signs, led to initial diagnostic delay. The combination of stroke, endocarditis, and necrotizing pneumonia from pneumococcus is exceedingly rare and not well documented in patients this young.
Recommendations/Conclusions: Austrian syndrome should be considered in patients presenting with systemic infection and multifocal involvement of the CNS, lungs, and heart—especially with S. pneumoniae bacteremia. Early echocardiography and neuroimaging are critical. Prompt antibiotic therapy and surgical evaluation for valve replacement are essential to improving outcomes.