internal medicine Sinai Hospital Of Baltimore baltimore, Maryland, United States
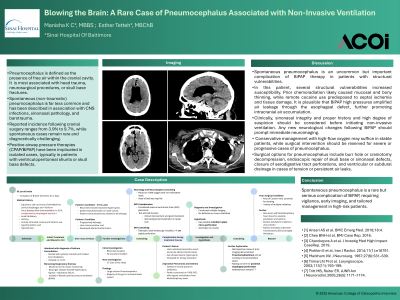
Clinical Scenario or Case: A 65-year-old man was admitted with severe asthma exacerbation and acute on chronic hypercapnic respiratory failure, requiring BiPAP in the ICU. His history included treated squamous cell carcinoma of the cervical esophagus and pyriform sinus (TxN1M0) with chemoradiation causing esophageal stenosis, plus remote tobacco and cocaine use, hypothyroidism, and hypertension. He also reported chronic nasal discomfort without other symptoms. After 3 hours of BiPAP, about 24 hours post-therapy, he developed lethargy, tachypnea, and confusion. Head CT showed extensive intraventricular pneumocephalus without CNS defects identified.
Evidence/Literature Review: Pneumocephalus occurs in about 3.9% to 9.7% of patients after cranial surgery, especially involving the posterior fossa or cranial base. It is less common after head trauma and rarely life-threatening unless tension pneumocephalus develops. A 2014 review by Pishbin et al. (cited in Ansari et al., 2018) found only 11 reported cases of spontaneous pneumocephalus, with causes including congenital skull base defects, infections, or sinus disease. In the context of CPAP use, spontaneous pneumocephalus is extremely rare, with only a few cases reported over past two decades.
Unique Aspects of Case: This case highlights spontaneous pneumocephalus after brief BiPAP use, without trauma, surgery, or infection. Imaging showed no skull base defects, but nasal endoscopy found a septal perforation likely allowing air entry worsened by positive pressure. The patient’s prior chemoradiation for esophageal and pyriform sinus cancer probably caused mucosal and bone thinning, while past cocaine use may have further damaged the nasal septum and skull base. Together with BiPAP pressure, these factors likely created a one-way valve effect, causing this rare condition.
Recommendations/Conclusions: Although spontaneous pneumocephalus as a rare but clinically significant complication of BiPAP therapy. This report underscores the need for heightened clinical vigilance when initiating positive pressure ventilation, especially in patients with known or suspected underlying nasal structural abnormalities and seeks to increase literature available in this regard.