Internal Medicine Oklahoma State University Medical Center Broken Arrow, Oklahoma, United States
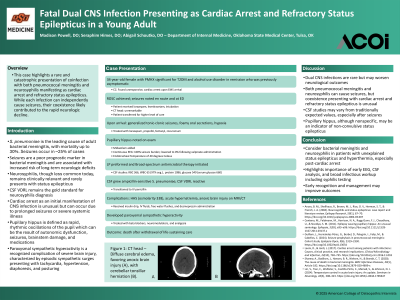
Clinical Scenario or Case: A 34-year-old woman, who was asymptomatic in the preceding days, was found unresponsive and in cardiac arrest at home. ROSC was achieved after bystander CPR. During EMS transport and at the referring ED, she had seizure-like activity and was treated with lorazepam, levetiracetam, and intubation. Head CT was unremarkable.
Upon transfer, she had generalized tonic-clonic seizures, foamy oral secretions, and hypoxia despite maximal ventilator support. She was sedated and paralyzed. Despite cessation of visible seizure activity, pupillary hippus persisted. Continuous EEG showed 100% seizure burden, which resolved after valproate administration. Her core temperature was notably 40°C. A lumbar puncture was performed, and empiric meningitis treatment was started. CSF culture grew S. pneumoniae, and CSF VDRL was reactive, confirming neurosyphilis. She was transitioned to IV penicillin.
Her course was complicated by hyperosmolar hyperglycemic syndrome, hypernatremia, and imaging evidence of anoxic brain injury. She later developed paroxysmal sympathetic hyperactivity. Despite aggressive care, she succumbed to severe anoxic injury and passed following withdrawal of life-sustaining measures.
Evidence/Literature Review: Streptococcus pneumoniae meningitis is associated with seizures in approximately 25% of cases. While neurosyphilis may present with varied neurologic symptoms, status epilepticus is rare. Cardiac arrest as the initial manifestation of central nervous system (CNS) infection is also uncommon. This case describes a fatal and atypical presentation of dual CNS infection.
Unique Aspects of Case: This case highlights a rare and catastrophic presentation of dual CNS infections manifesting as cardiac arrest and refractory status epilepticus. While each infection can independently cause seizures, their coexistence likely contributed to the rapid neurologic decline.
Recommendations/Conclusions: In cases of unexplained status epilepticus and hyperthermia, particularly after cardiac arrest, clinicians should maintain a broad differential that includes both bacterial meningitis and neurosyphilis. Additionally, pupillary hippus may be an indicator of non-convulsive status epilepticus. Early EEG monitoring, CSF analysis, and broad infectious workup—including for syphilis—are critical.