(56-STU) Clinical efficacy of Nivolumab monotherapy, Ipilimumab monotherapy, and combined Nivolumab and Ipilimumab therapy in BRAF-mutant vs BRAF-wild type melanoma, a meta-analysis
Osteopathic Medical Student Lincoln Memorial University DeBusk College of Osteopathic Medicine Henderson, Kentucky, United States
Introduction/Background: Nivolumab and Ipilimumab are immune checkpoint inhibitors (ICIs) widely used in the treatment of Melanoma. Nivolumab binds to the programmed death-1 (PD-1) receptor on T-cells preventing interaction with the PD-1 ligands, while ipilimumab binds to cytotoxic T-lymphocyte associated antigen 4 (CTLA-4), blocking its interaction with B7 molecules on antigen-presenting cells. By preventing inhibitory signals that suppress T cell activity, these mechanisms promote T cell activation, resulting in a sustained anti-tumor response. BRAF is a serine/threonine-protein kinase involved in the regulation of cell growth and survival. Mutations in BRAF are seen in many malignancies, including melanoma.
Methods: To investigate the clinical efficacy of nivolumab monotherapy, ipilimumab monotherapy, and combined nivolumab and ipilimumab therapy in patients with BRAF-mutant and BRAF-wild type melanoma, a meta-analysis was conducted on published studies containing clinical outcomes of these treatments. Published studies of the clinical efficacy of nivolumab monotherapy, ipilimumab monotherapy, and combined nivolumab with ipilimumab were collected through PubMed. Studies focusing on a specific melanoma subtype or brain metastasis were excluded. Objective response rate (ORR), progression free survival (PFS), and overall survival (OS) were assessed to determine clinical efficacy. After screening for studies with similar methodologies, a total of 18 studies were included.
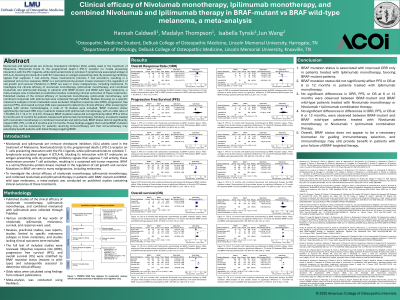
Results/Discussion: BRAF mutation status significantly improved ORR only in patients treated with ipilimumab monotherapy, with an odds ratio of 1.78 (95% CI: 1.15-2.77, p=0.01). However, BRAF mutation status did not significantly affect PFS or OS at 6 months and 12 months for patients treated with ipilimumab monotherapy. Similarly, in patients treated with nivolumab monotherapy or combined nivolumab and ipilimumab, BRAF status did not significantly impact ORR, PFS, or OS at 6 months and 12 months.
Conclusions: These findings suggest that routine BRAF mutation testing may not be necessary for patients receiving immunotherapy and that immunotherapy may potentially benefit patients with failed therapy targeting BRAF.