(34-RES) The Underestimated Danger of Congenital Hypothyroidism in Adulthood: A Case of Massive Pericardial Effusion in an Adult with Untreated Congenital Hypothyroidism.
Internal Medicine OhioHealth Doctors Hospital Powell, Ohio, United States
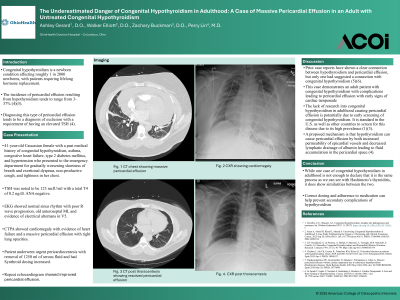
Clinical Scenario or Case: Patient was a 41-year-old Caucasian female with a past medical history of congenital hypothyroidism, asthma, anemia, congestive heart failure, type 2 diabetes mellitus, and hypertension who presented to the emergency department for gradually worsening shortness of breath, exertional dyspnea, intermittent nonproductive cough, and tightness in her chest. Her TSH was noted to be 123 mclU/ml with a total T4 of 0.2 ng/dl. EKG showed normal sinus rhythm with poor R wave progression, old anteroseptal MI, and evidence of electrical alternans in V5. The CTPA showed cardiomegaly with evidence of heart failure and a massive pericardial effusion with right lung opacities. Patient underwent urgent pericardiocentesis with removal of 1250 ml of serous fluid. Synthroid dosing was increased to 200 mcg which helped improve her thyroid hormone levels. Repeat echocardiogram showed improved pericardial effusion. ANA testing was negative, ruling out other autoimmune causes for pericardial effusion, suggesting hypothyroidism as the leading contributor to the pericardial effusion.
Evidence/Literature Review: Congenital Hypothyroidism is a newborn condition affecting roughly 1 in 2000 newborns, with patients requiring lifelong hormone replacement. The incidence of pericardial effusion resulting from hypothyroidism tends to range from 3-37% (4)(5). Diagnosing this type of pericardial effusion tends to be a diagnosis of exclusion with a requirement of having an elevated TSH (4). It is believed that hypothyroidism can cause pericardial effusion by both increased permeability of epicardial vessels and decreased lymphatic drainage of albumin leading to fluid accumulation in the pericardial space (4).
Unique Aspects of Case: Prior case reports have shown a connection between hypothyroidism and pericardial effusion, but very little have suggested a connection with congenital hypothyroidism (5)(6).
Recommendations/Conclusions: While one case of congenital hypothyroidism in adulthood is not enough to declare that it is the same process as we can see with Hashimoto's thyroiditis, it does show similarities between the two.