IM Canyon Vista Medical Center Sierra Vista, Arizona, United States
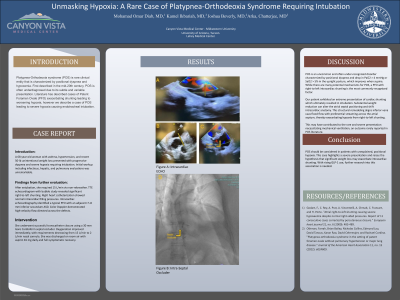
Clinical Scenario or Case: A 68-year-old woman with asthma, hypertension, and recent 50-lb unintentional weight loss presented with progressive dyspnea and severe hypoxia requiring intubation. Initial workup including infectious, hepatic, and pulmonary evaluations was unremarkable. After extubation, she required 15 L/min via non-rebreather. TTE echocardiogram with bubble study revealed significant right-to-left shunting. Right heart catheterization showed normal intracardiac filling pressures. Intracardiac echocardiography identified a typical PFO with an adjacent 7–8 mm inferior secundum ASD. Color Doppler demonstrated high-velocity flow directed across the defects. She underwent successful transcatheter closure using a 30 mm Gore Cardioform septal occluder. Oxygenation improved immediately, with requirements decreasing from 15 L/min to 2 L/min nasal cannula.
Evidence/Literature Review: POS is an uncommon and often under-recognized disorder characterized by positional dyspnea and drop in PaO2 > 4 mmHg or SaO2 > 5% in the upright posture, which improves when supine. While there are many potential mechanisms for POS, a PFO with right-to-left intracardiac shunting is the most commonly recognized factor. Our patient exhibited an extreme presentation of cardiac shunting which ultimately resulted in intubation. Substantial weight reduction can alter the atrial septal positioning and shift intracardiac anatomy. This structural remodeling aligns inferior vena cava flood flow with preferential streaming across the atrial septum, thereby exacerbating hypoxia from right-to-left shunting. This may have contributed to the rare and severe presentation necessitating mechanical ventilation—an outcome rarely reported in POS literature.
Unique Aspects of Case: POS is well known to cause Hypoxia in patients, however we present a rare case in which a patient required rapid sequence intubation due to POS.
Recommendations/Conclusions: POS should be considered in patients with unexplained, positional hypoxia. This case highlights a severe presentation and raises the hypothesis that significant weight loss may exacerbate intracardiac shunting. With rising GLP-1 use, further research into this association is needed.