Internal Medicine Midwestern University - Canyon Vista Medical Center Tucson, Arizona, United States
Clinical Scenario or Case: We report a case of a 62-year-old man recently treated for presumed otitis media and periorbital cellulitis, who presented with headache, vertigo, ataxia, and worsening hearing loss. Computed tomography of the head was unremarkable. Brain MRI demonstrated diffuse dural and meningeal enhancement, consistent with pachymeningitis. CSF fluid had WBC of 12 with 36% monocytes; cytology and flow-cytometry were unremarkable. Repeat MRI/MRV showed diffuse pachymeningeal enhancement, with dural involvement of the right internal auditory canal. He had rapidly progressive bilateral facial palsy and worsening of sensorineural hearing loss. He had non-necrotizing diffuse scleritis on ophthalmology evaluation for conjunctival injection. Neurosurgical meningeal biopsy revealed acute and chronic inflammation without granulomas. An initial working diagnosis of neurosarcoidosis was made, and he received high-dose corticosteroids with modest improvement. He was discharged on oral prednisone, later initiated on methotrexate, then adalimumab. Due to hepatotoxicity, Methotrexate was switched to mycophenolate, which resulted in marked clinical improvement. Given the absence of granulomatous inflammation and marked response to mycophenolate, the diagnosis was refined to Cogan’s Syndrome. Follow-up MRI demonstrated resolution of dural thickening. As of 07/2025, patient remains stable on adalimumab and mycophenolate, without flare-ups
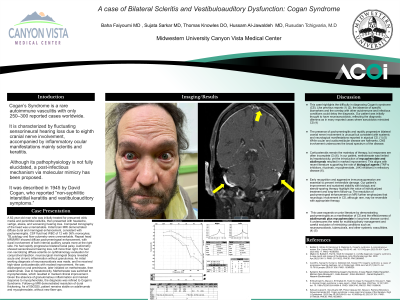
Evidence/Literature Review: Cogan’s Syndrome is a rare autoimmune vasculitis with only 250–300 reported cases worldwide. It is characterized by fluctuating sensorineural hearing loss due to eighth cranial nerve involvement, accompanied by inflammatory ocular manifestations. Although its pathophysiology is not fully elucidated, a post-infectious mechanism via molecular mimicry has been proposed. It was described in 1945 by David Cogan, who reported “non-syphilitic interstitial keratitis and vestibuloauditory symptoms.”
Unique Aspects of Case: In this case, the patient's initial presentation mimicked Neurosarcoidosis; however, the course of response to the treatment made Cogan Syndrome a more reasonable diagnosis
Recommendations/Conclusions: Cogan Syndrome is an uncommon autoimmune vasculitis affecting cranial nerves—particularly VIII—and ocular tissues. It may closely mimic neurosarcoidosis, necessitating careful clinicopathologic correlation for accurate diagnosis.