Internal Medicine Fairfield Medical Center Columbus, Ohio, United States
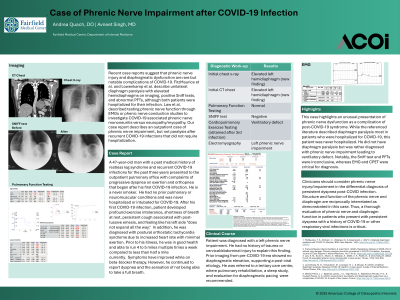
Clinical Scenario or Case: A 47-year-old male with recurrent COVID-19 infections presented with progressive dyspnea on exertion and orthopnea. He had no prior pulmonary or neuromuscular conditions and was never hospitalized or intubated for COVID-19. Chest CT revealed elevation of the left hemidiaphragm. Pulmonary function testing and Sniff test were negative for diaphragmatic paralysis. Cardiopulmonary exercise testing (CPET), obtained after his third infection, demonstrated a ventilatory defect. Electromyography (EMG) revealed findings consistent with left phrenic nerve impairment. The patient had no history of trauma or cervical/abdominal injury, and prior imaging from 2018 showed no diaphragmatic elevation, supporting a post-viral etiology. He was referred to a tertiary center, where pulmonary rehabilitation, a sleep study, and evaluation for diaphragmatic pacing were recommended.
Evidence/Literature Review: Recent case reports suggest that phrenic nerve injury and diaphragmatic dysfunction are rare but notable complications of COVID-19. FitzMaurice et al. and Lowenkamp et al. describe unilateral diaphragm paralysis with elevated hemidiaphragms on imaging, positive Sniff tests, and abnormal PFTs, although both patients were hospitalized for their infection. Law et al. described testing phrenic nerve function through EMGs or phenic nerve conduction studies to investigate COVID-19 associated phrenic nerve mononeuritis versus neuropathy/myopathy.
Unique Aspects of Case: This case highlights an unusual presentation of phrenic nerve dysfunction as a complication of post-COVID-19 syndrome. While the referenced literature described diaphragm paralysis most in patients who were hospitalized for COVID-19, this patient was never hospitalized. He did not have diaphragm paralysis, but was rather diagnosed with phrenic nerve impairment. Notably, the Sniff test and PFTs were inconclusive, whereas EMG and CPET were critical for diagnosis.
Recommendations/Conclusions: Clinicians should consider phrenic nerve injury in the differential diagnosis of persistent dyspnea post-COVID infection. This case demonstrates the importance of thorough evaluation of diaphragm function in patients who present with persistent dyspnea with a history of COVID-19 or other respiratory viral infections.