Introduction: Spinal epidural abscess (SEA) is a rare but life-threatening condition often caused by hematogenous spread of Staphylococcus aureus. Early recognition and intervention are critical to prevent permanent neurological deficits.
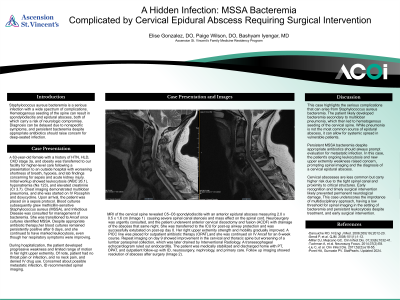
Case Presentation: We present a 63-year-old female with a history of hypertension, hyperlipidemia, CKD3a, and obesity who was admitted with sepsis secondary to multilobar pneumonia and persistent MSSA bacteremia. Despite broad-spectrum antibiotics, she developed progressive right upper extremity weakness. MRI revealed C5–C6 spondylodiscitis with an anterior epidural abscess causing severe canal stenosis. She underwent emergent anterior cervical discectomy and fusion with abscess drainage, followed by targeted IV cefazolin therapy. Repeat imaging demonstrated improvement of the cervical abscess but revealed a new lumbar abscess requiring IR-guided drainage. She completed an 8-week course of IV antibiotics via PICC line and recovered with improved neurological function.
Evidence/Literature Review: Darouiche RO. N Engl J Med. 2006;355(19):2012-20. Sendi P, et al. QJM. 2008;101(1):1-12. Miller DJ, Mejicano GC. Clin Infect Dis. 2001;33(6):1032-41. Tuchman A, et al. Neurosurg Focus. 2014;37(2):E8. Liu C, et al. Clin Infect Dis. 2011;52(3):e18-55. Poret HA, Gumaste PV. StatPearls. Updated 2024.
Unique Aspects of Case: This case highlights hematogenous seeding of the spine from a pulmonary source leading to SEA, emphasizing the importance of considering spinal infection in patients with MSSA bacteremia and new neurological symptoms. Prompt diagnosis through MRI and timely surgical intervention are essential to optimize outcomes.
Recommendations/Conclusions: SEA should be suspected in bacteremic patients with neurological deficits, even when the primary infection is distant. Early multidisciplinary management—including infectious disease, neurosurgery, and interventional radiology—is key to reducing morbidity.