Internal Medicine University of Tennessee Medical Center Knoxville, Tennessee, United States
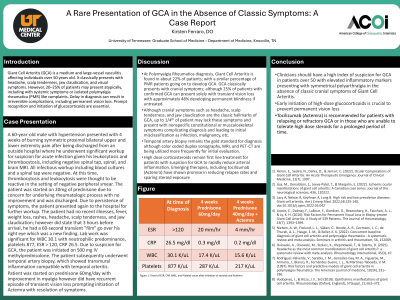
Clinical Scenario or Case: A 60-year-old male with hypertension presented with 4 weeks of burning symmetric bilateral upper and lower extremity pain after being discharged from an outside hospital where he underwent significant workup, including negative spinal and brain MRI. On laboratory workup, patient was found to have leukocytosis and thrombocytosis, initially thought to be related to acute infection; however, all infectious workup, including blood cultures and a spinal tap were negative. At this time, the patient was started on 20mg of prednisone due to concern for underlying rheumatologic process with no improvement. Due to persistence of symptoms, the patient presented again to the hospital for further workup. The patient has no recent illnesses, fever, weight loss, rashes, headache, scalp tenderness, and jaw claudication; however did state that 3 hours before arrival, he had a 60-second transient "film" go over his right eye. Lab work was significant for WBC 30.1 with neutrophilic predominance, platelets 877, ESR > 120, CRP 26.5. Due to suspicion for GCA, the patient was initiated on 500 mg IV methylprednisolone. The patient subsequently underwent temporal artery biopsy, which showed transmural inflammation compatible with temporal arteritis.
Evidence/Literature Review: At PMR diagnosis, GCA is found in about 22% of patients; with a similar percentage of PMR patients going on to develop PMR. GCA classically presents with cranial symptoms; although 25% of patients with confirmed GCA can present solely with transient vision loss with approximately 48% developing permanent blindness if untreated.
Unique Aspects of Case: Our case highlights an atypical presentation of biopsy-proven GCA in which there was an absence of hallmark cranial features of GCA.
Recommendations/Conclusions: Clinicians should have a high index of suspicion for GCA in patients over 50 with elevated inflammatory markers presenting with symmetrical polyarthralgia in the absence of classic cranial symptoms of GCA, as early treatment is essential to prevent permanent visual loss.