IM University of Miami Cooper City, Florida, United States
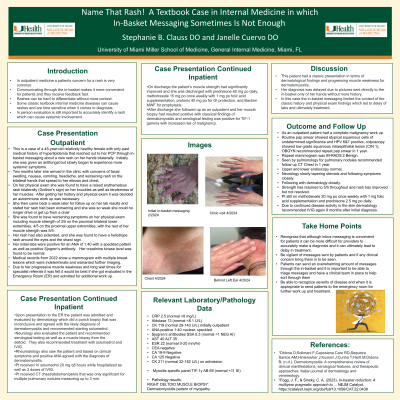
Clinical Scenario or Case: This is a case of a 45-year-old relatively healthy female with only PMH of hyperlipidemia that reached out to her PCP through inbasket messaging about a new rash on her hands bilaterally. Initially she was given an antifungal but slowly began to experience more systemic symptoms such as muscle weakness and aches. She arrived in the clinic with concerns of worsening rash. On her PE she was found to have a raised erythematous rash bilaterally on the elbows and knuckles. After exam and history it was decided a dermatomyositis work up was necessary. She then came back for follow up on her lab results and was found to have worsening symptoms on exam . Her rash had also extended and she was found to have a heliotrope rash around the eyes bilaterally and the shawl sign. Her labs were positive for an ANA of 1:40 with a speckled pattern as well as positive Sjogren's. Due to her worsening she was sent to the ER, the patient was admitted and evaluated by dermatology and agreed with the likely diagnosis of dermatomyositis and recommended starting solumedrol and IVIG. On discharge the patients muscle strength had significantly improved. After discharge she followed up with me her muscle biopsy which resulted positive for dermatomyositis and serological testing was positive for TIF 1 gamma with increased risk of malignancy. Complete malignancy work up was done and negative.
Evidence/Literature Review: Dermatomyositis on pubmed
Unique Aspects of Case: This case demonstrates how getting histories and doing physical exams are the standard of care for patients.
Recommendations/Conclusions: Her diagnosis was delayed due to pictures sent directly to the in-basket only of her hands. In this case the in-basket messaging limited the context of the classic physical exam findings which led to delay of labs and ultimately treatment.