Internal Medicine and Osteopathic Manipulative Medicine Campbell University Buies Creek, North Carolina, United States
Background: Importance: Complementary health approaches (CHAs) are increasingly integrated into US healthcare, yet updated nationally representative data on prevalence and demographic disparities across distinct CHA categories remain limited. Understanding these patterns is critical for informing equitable policy and clinical integration.
Objective: To assess the 12-month prevalence of CHA use among US adults and identify demographic predictors associated with CHA participation.
Methods: Design, Setting, and Participants: This cross-sectional study analyzed a nationally representative survey of 3022 US adults conducted in August 2024. Participants were quota-sampled to match 2024 Census benchmarks. Exclusions included incomplete CHA or demographic data. Exposures: Demographic variables: age, sex, race/ethnicity, education, employment, income, insurance status, geographic region, and residence. Primary Outcomes and Measures: Self-reported CHA use (yes/no) within the past 12 months, across five categories. Weighted prevalence estimates and adjusted odds ratios (AORs) from logistic regression models identified predictors (α = 0.05).
Results:
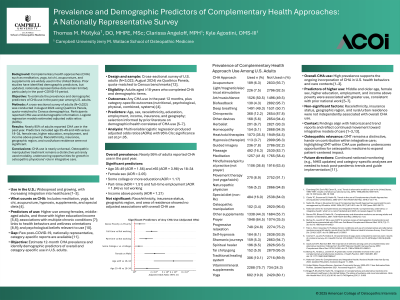
Results: Among 3022 participants (median age 48 years [IQR 33–61]; 50.3% female), 94.8% (95% CI 93.6–95.8) reported using ≥1 CHA. Prevalence by category: N-CHA (81.1%), Ps-CHA (80.2%), C-CHA (63.5%), Ph-CHA (24.0%), S-CHA (12.3%). Key predictors included age, sex, education, and employment. Adults ≥65 years had higher Ps-CHA use (AOR 1.67 [1.21–2.31], P = .002) when compared to the 18–34 year group. Females had higher Ps-CHA use (AOR 2.04 [1.52–2.74], P < .001). College-educated individuals had higher Ph-CHA use (AOR 1.49 [1.22–1.81], P < .001). Full-time workers had higher C-CHA use (AOR 1.33 [1.08–1.64], P = .008). Geographic region and insurance status showed no significant associations.
Conclusions: Conclusions and Relevance: Nearly all US adults reported CHA use, with significant disparities by age, sex, education, and employment. Policymakers and clinicians must address barriers to equitable access, prioritize evidence-based CHA integration, and improve patient-provider communication to align care with population health behaviors.