Student Pacific Northwest University Tacoma, Washington, United States
Clinical Scenario or Case: A middle-aged woman with untreated low-grade B-cell lymphoma, a remote diagnosis of severe psoriatic arthritis, and valvular heart disease presented with several weeks of progressive exertional dyspnea and unintentional weight loss. Her history also included multiple prior hospitalizations for erosive arthropathy with toe autoamputation. The current physical exam revealed a systolic murmur, severe hand and foot deformities, and numerous papular and nodular skin lesions on her extremities and face. Additional findings included corneal changes and peripheral neuropathy. Echocardiogram showed diffuse valve thickening, severe aortic stenosis, and heart failure with reduced ejection fraction. Prior records noted MYD88-positive lymphoplasmacytic lymphoma diagnosed several years prior but managed with observation due to lack of cytopenias or concerning symptoms.
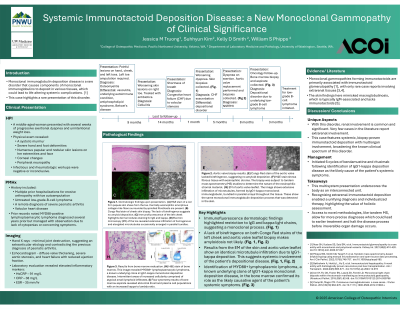
During this admission, infectious and rheumatologic workups were unrevealing. Notably, hand X-rays showed minimal joint destruction, suggesting an extraarticular etiology and contradicting the previous diagnosis of psoriatic arthritis. Biopsy of a skin lesion showed dermal amorphous eosinophilic nodules, and an aortic valve biopsy showed expansion of the leaflet by amorphous eosinophilic material. Congo Red staining was negative for amyloid. We performed tandem mass spectrometry [1] and electron microscopy to identify monoclonal IgG1 kappa deposition forming microtubular structures, termed “immunotactoids,” at both sites. Based on these findings, the untreated lymphoplasmacytic lymphoma was suspected as the underlying cause of the holistic picture, leading to initiation of clone-directed therapy.
Evidence/Literature Review: Monoclonal gammopathies forming immunotactoids are primarily associated with immunotactoid glomerulopathy [2], with only rare case reports involving extrarenal tissues [3,4]. The skin findings here mimicked macroglobulinosis, which is typically IgM-associated and lacks immunotactoids [5].
Unique Aspects of Case: This case features systemic, biopsy-proven immunotactoid deposition with multiorgan involvement, broadening the known clinical spectrum of this disorder.
Recommendations/Conclusions: This multisystem presentation underscores the body as an interconnected unit. Recognizing extrarenal immunotactoid deposition enabled a unifying diagnosis and individualized therapy, highlighting the value of holistic assessment.