Third year medical student Rowan-Virtua School Of Osteopathic Medicine Edison, New Jersey, United States
Introduction/Background: Antiretroviral therapy (ART) has dramatically improved survival among women living with HIV; however, it is associated with an increased risk of cardiovascular disease (CVD). This vulnerability is especially concerning for women who already face additional CVD risk due to hormonal, metabolic, and immune factors. ART may further exacerbate atherosclerosis, insulin resistance, and inflammatory pathways, while socioeconomic determinants and healthcare access barriers compound these vulnerabilities. This systematic review identified key factors contributing to increased cardiovascular risk in women with HIV on ART, with the goal of developing a targeted patient survey as a quality improvement measure to enhance clinical risk assessment, support individualized care management, and guide future research on patient-centered prevention strategies.
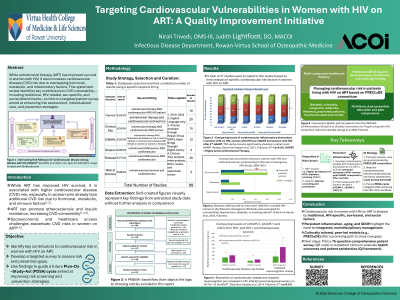
Methods: A systematic search across five major databases was conducted using targeted keyword strings relating to antiretroviral therapy, cardiovascular disease, and women. Twenty-one studies were ultimately included after screening and extraction of relevant data. Extracted data were organized and displayed using PRISMA flow diagrams and self-created figures summarizing relevant biomarkers and comorbidities.
Results/Discussion: Four major domains emerged as contributors to cardiovascular vulnerability in this population: traditional risk factors, HIV-specific risk factors, sex-specific risk factors, and social determinants of health (SDOH). Elevated inflammatory markers, including TNF-alpha, persisted post-ART and were associated with increased CVD risk. Comorbidities, hypertension burden, and biomarkers of endothelial dysfunction (e.g., sVCAM-1, sICAM-1) were also elevated in women living with HIV on ART compared to controls. Frameworks such as the PRECluDE consortium emphasize culturally tailored, trauma-focused, multicomponent prevention strategies to address these intersecting risk pathways.
Conclusions: Cardiovascular risk among women on ART is multifactorial, requiring management strategies that integrate traditional, HIV-related, sex-based, and SDOH influences. Further investigation is warranted, particularly in postmenopausal women with HIV. A patient-centered survey has been developed to further explore these risk perceptions and to guide future prevention efforts.