Internal Medicine Arizona College of Osteopathic Medicine Phoenix, Arizona, United States
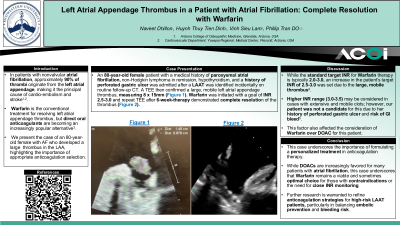
Clinical Scenario or Case: An 80-year-old female patient with a medical history of paroxysmal atrial fibrillation, non-Hodgkin lymphoma in remission, hypothyroidism, and a history of perforated gastric ulcer was admitted after a LAAT was identified incidentally on routine follow-up CT. A TEE then confirmed a large, mobile left atrial appendage thrombus, measuring 8 x 15mm. Warfarin was initiated with a goal of INR 2.5-3.0, and repeat TEE after 6-week-therapy demonstrated complete resolution of the thrombus.
Evidence/Literature Review: In patients with nonvalvular atrial fibrillation, approximately 90% of thrombi originate from the left atrial appendage, making it the principal cause of cardioembolism and stroke. Warfarin is the conventional treatment for resolving left atrial appendage thrombus, but direct oral anticoagulants are becoming an increasingly popular alternative. Here, we represent the case of an 80-year- old female with AF and no prior anticoagulation history, who developed a massive thrombus in the LAA, highlighting the importance of appropriate anticoagulation selection.
Unique Aspects of Case: While the standard target INR for Warfarin therapy is typically 2.0-3.0, a slight increase in patient’s target INR of 2.5-3.0 was set due to the large, mobile thrombi and elevated CHA2DS2-VA score. Higher INR range (3.0-3.5) may be considered in cases with extensive and mobile clots; however, our patient was not a candidate for this due to her history of perforated gastric ulcer and risk of GI bleed. This factor also affected the consideration of warfarin over DOAC for this patient.
Recommendations/Conclusions: This case underscores the importance of formulating a personalized treatment in anticoagulation therapy. While mounting evidence for the preferable use of DOACs over Warfarin in atrial fibrillation patients with LAAT is being produced by large clinical trials, patient-specific risk factors remain pivotal to guiding therapeutic management.