(63-STU) Outcomes and Disparities in Cardiothoracic Surgical Patients With and Without Major Complications or Comorbidities (MCC) During COVID-19 Hospitalizations: A National Analysis Using the NIS Database
Medical Student Future Forwards Research Institute Fair Lawn, New Jersey, United States
Introduction/Background: Gender, viruses, and sociodemographic information all play a role in determining outcomes in patients presenting with cardiothoracic issues. This study aims to explore the different variables that impact survivability in those presenting with cardiothoracic procedures and labeled with major complications and comorbidities (MCC) within the NIS 2020 database.
Methods: 189,540 adult hospitalizations for cardiothoracic surgery were analyzed from the 2020 NIS database. Length of stay (LoS) was analyzed on the natural-log scale, a weighted logistic model was used to analyze the dominant risk factors, and crude χ² comparisons analyzed mortality by demographic characteristics.
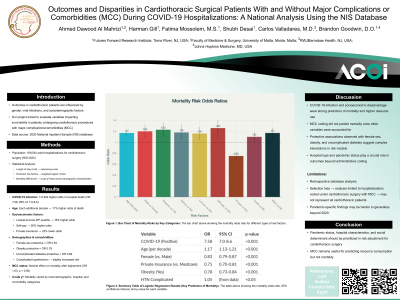
Results/Discussion: COVID-19 infection multiplied the odds of in-hospital death 7.6-fold (OR 7.58, 95% CI 7.0–8.6). Each additional decade of age increased the odds by 17%. Patients from the lowest-income ZIP-code quartile and those self-paying had 16% and 26% higher odds of death, whereas privately insured patients had 25% lower odds. Crude χ² comparisons confirmed that mortality differed by most demographic, hospital, and comorbidity categories. Although they remained conventional “with-MCC”. Female (OR 0.83), uncomplicated diabetes (OR 0.69), and obesity (OR 0.78) were independently protective. Complicated hypertension raised risk slightly, but the presence of any MCC-coded DRG remained neutral (OR 1.03, p = 0.50) once other factors were controlled.
Conclusions: The data indicated that the presence of COVID-19 infection in teaching hospitals and socio-economic disadvantaged areas had increased death rates, longer LOS, and higher cost than the traditional “with-MCC” classification. MCC did not predict mortality once these factors were considered, but it remained a reliable marker of excess resource consumption. The analysis suggests that pandemic status, hospital characteristics and modifiable social variables should be central to risk adjustment and quality-improvement efforts in cardiothoracic surgery, rather than relying solely on administrative MCC labels.