Medical Student Alabama College of Osteopathic Medicine Coral Springs, Florida, United States
Introduction/Background: Chronic pain is one of the most common and debilitating comorbidities faced by people living with HIV, affecting more than half of this population over their lifetime. This study evaluates the contribution of non-antiretroviral medications to pain outcomes in people with HIV.
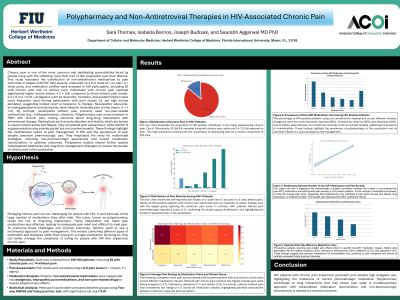
Methods: Pain severity, measured on a 0–5 scale (0 = no pain; 5 = worst pain), and medication profiles were analyzed in 106 participants, including 92 with chronic pain and 14 without pain.
Results/Discussion: Individuals with chronic pain reported significantly higher scores (mean: 4.2 ± 0.8) compared to those without pain (mean: 0.4 ± 0.3; p < 0.01). Analgesics such as ibuprofen, tramadol, and acetaminophen were most frequently used among participants with pain scores ≥4, yet high scores persisted, suggesting limited relief or tolerance to therapy. Neuropathic adjuvants, including gabapentin and duloxetine, were linked to moderate pain scores (mean: 3.1 ± 1.0). By contrast, participants without pain primarily used non-pain-related medications (e.g., antihypertensives, vitamins). Polypharmacy was more prevalent in PWH with chronic pain, raising concerns about drug–drug interactions with antiretroviral therapy. Medications like beta-blockers and statins, known to cause muscle aches and fatigue, may complicate pain assessment, while vitamin D supplementation may provide partial but not curative benefits. These findings highlight the multifaceted nature of pain management in HIV and the persistence of pain despite extensive pharmacologic use.
Conclusions: They emphasize the need for multimodal strategies, including non-pharmacologic approaches and careful medication reconciliation, to optimize outcomes. Prospective studies should further explore individualized treatments and long-term management strategies to reduce the burden of chronic pain in this population.