resident internal medicine sinai hospital of baltimore Baltimore, Maryland, United States
Clinical Scenario or Case: A 64-year-old male with a history of coronary artery disease and hypertension presented with bilateral lower limb weakness and urinary retention for 2 days. .On evaluation, he was found to have a lumbar epidural abscess and newly developed left-sided mitral valve vegetation, consistent with infective endocarditis.
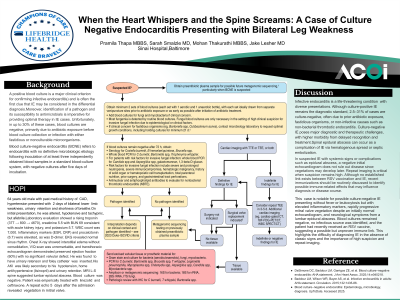
Evidence/Literature Review: Infective endocarditis is a life-threatening condition with varied presentations. While culture-positive IE remains the standard diagnostic pathway, up to 2.5–31% of cases are culture negative, often due to prior antibiotic exposure, fastidious organisms, or non-infective etiologies such as non-bacterial thrombotic endocarditis. Culture-negative IE poses significant diagnostic and therapeutic challenges and is associated with higher morbidity due to delayed identification and treatment initiation. Spinal epidural abscess has been reported as a complication of Infective endocarditis, either via hematogenous spread or septic embolization
Unique Aspects of Case: This case is unique due to culture-negative infective endocarditis presenting without fever or leukocytosis but with elevated inflammatory markers, rapid development of mitral valve vegetation after a negative initial echo, and neurological symptoms from a lumbar epidural abscess likely seeded from the heart. Blood cultures remained negative, no infection source was found, and the patient had received an RSV vaccine two days before symptoms began, suggesting a possible but unproven immune link. This highlights the challenge of diagnosing endocarditis without classic signs and the importance of high suspicion and repeat imaging.
Recommendations/Conclusions: In suspected infective endocarditis, especially with systemic signs or complications like epidural abscess, a negative initial transthoracic echo doesn’t exclude diagnosis since vegetations can develop later. Repeat imaging, is crucial when suspicion remains high. Although no link exists between RSV vaccination and endocarditis, recent vaccinations should be routinely asked about to identify possible immune-related effects that could affect diagnosis or clinical course