Student Michigan State College of Osteopathic Medicine Detroit, Michigan, United States
Clinical Scenario or Case: A 73 year old female with a past medical history of asthma, cardiac ablation, anemia, total hip arthroplasty, and history of hiatal hernia status post repair with Nissen fundoplication, presented for evaluation of sharp left-sided pain and acute shortness of breath. The patient reports following repair of her hernia 3 years ago, she has experienced dysphagia. She had previously been evaluated by surgery and gastroenterology, with negative EGD. She denied overt aspiration or choking, complications post recent dental procedure, or recent upper respiratory illness. She also denied fever, chills, or sputum production. Laboratory workup demonstrated white blood cell count of 29.6 with left shift. In the Emergency department, she was found to have loculated L sided pleural effusion on CT scan and a chest tube was placed, with greater than 1L of pleural fluid removed.
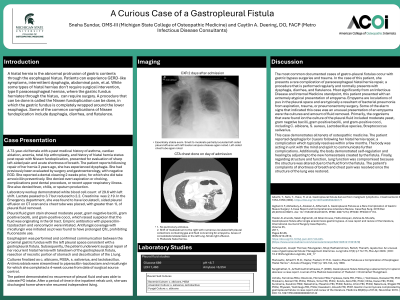
Pleural fluid gram stain showed moderate yeast, gram negative bacilli, gram positive bacilli, and gram positive cocci, which raised suspicion that the fluid was originating in the GI tract. Empiric antibiotics with piperacillin-tazobactam and vancomycin were initiated. Antifungal coverage with micafungin was initiated as pt was found to have prolonged QTc, prohibiting fluconazole use.
Esophagram was performed and confirmed communication between the proximal gastric fundus with the left pleural space consistent with a gastropleural fistula.
Evidence/Literature Review: Gastro-pleural fistulas are more commonly associated with gastric bypass surgeries and trauma.
Unique Aspects of Case: This case demonstrates a rare complication of paraesophageal hiatal hernia that recurred and resulted in gastro-pleural fistula. While initial imaging findings were consistent with loculated empyema, typically associated with aspiration events or bacterial pneumonias, the microbiologic findings in the culture were more consistent with a gastrointestinal origin.
Recommendations/Conclusions: Subsequently, the patient underwent surgical repair of her recurrent hiatal hernia with takedown of the gastropleural fistula, resection of necrotic portion of stomach and decortication of the L lung.