Internal Medicine Nova Southeastern University Davie, Florida, United States
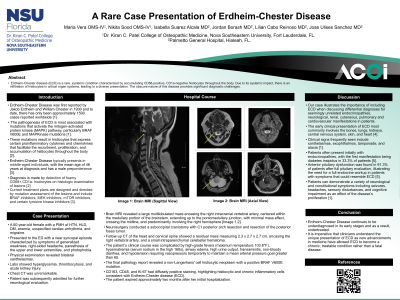
Clinical Scenario or Case: We present the case of a 60-year-old female patient with a past medical history of hypertension, diabetes mellitus, unspecified cardiac arrhythmia, and migraine who presented with generalized weakness, right-sided headache, and paresthesia of the extremities. Brain MRI reported a large multilobulated mass centered within the medullary portion of the brainstem. Histopathologic evaluation confirmed Erdheim-Chester disease (ECD) positive for the BRAF V600E mutation. The patient showed significant central nervous system involvement with associated endocrine, renal, and pulmonary involvement.
Evidence/Literature Review: Erdheim-Chester Disease (ECD) is a rare multisystem disease consisting of the proliferation of histiocytes originating from the myeloid cell line [1]. To date, there has only been approximately 1500 cases reported worldwide [2]. The pathogenesis of ECD is associated with mutations that activate the mitogen-activated protein kinase (MAPK) pathway [2]. Diagnosis is made by detection of foamy CD68+,CD1a- histiocytes on histologic examination of lesions [3]. Treatment is directed by mutation assessment of the lesions and include BRAF inhibitors, MEK inhibitors, mTOR inhibitors, and certain tyrosine kinase inhibitors [5].
Unique Aspects of Case: This patient’s diagnosis was prolonged due to decreased clinical suspicion of seemingly unrelated conditions. This patient developed a large medullary mass after years of demonstrating other systemic symptoms such as hypertension, hyperglycemia, leg pain, and xanthelasmas related to ECD. Her hydronephrosis and urinary retention indicated the histiocytic infiltration impacting the kidneys. If diagnosis had been made sooner, this patient may have been able to receive treatment opportunities to prolong life.
Recommendations/Conclusions: Our case illustrates the importance of including Erdheim-Chester Disease when discussing differential diagnoses for endocrinopathies that occur alongside neurological, nephrologic, cutaneous, pulmonary and cardiovascular manifestations in patients. Our case hopes to serve as an example of the seemingly unrelated symptoms produced by ECD in hopes of aiding the early diagnosis and treatment of this devastating disease.