Internal and Emergency Medicine Jefferson Health Northeast PHILADELPHIA, Pennsylvania, United States
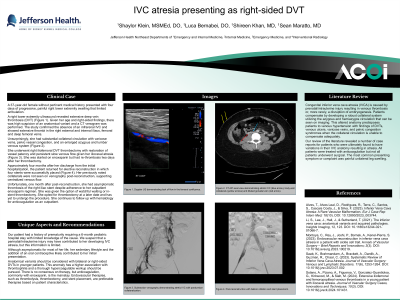
Clinical Scenario or Case: A 37-year-old female without any pertinent medical history presented with four days of progressive, painful right lower extremity swelling. Given her age and right-sided findings, there was high suspicion of an anatomical variant causing a DVT. CT venogram confirmed absence of an infrarenal IVC and extensive thrombi in the right external/internal iliac, femoral, and deep femoral veins. She had notable collateral circulation with varicose veins, pelvic vessel congestion, and an enlarged azygous venous system. Given her preference, she underwent interventional thrombectomy. She returned and received a successful iliocaval reconstruction. She had multiple episodes of re-thrombosis despite anticoagulation. Notably, she had a history of prematurity requiring a 6-month pediatric hospital stay with limited knowledge of the cause.
Evidence/Literature Review: Inferior vena cava atresia (IVCA) is caused by prenatal/intrauterine injury resulting in venous thrombosis or, more rarely, a disruption of embryogenesis. Patients compensate by developing a robust collateral system utilizing the azygous and hemiazygos circulation that can be seen on imaging. This altered anatomy predisposes patients to venous hypertension with findings of DVTs, venous ulcers, varicose veins, and pelvic congestion syndromes when the collateral circulation is unable to compensate adequately.
Unique Aspects of Case: Our patient likely had IVCA due to a perinatal/intrauterine injury given her childhood history, but this information is limited. Although asymptomatic for most of her life, her sedentary lifestyle and the addition of an oral contraceptive likely contributed to her presentation.
Recommendations/Conclusions: Anatomical variants should be considered with bilateral or right-sided DVTs in younger patients. This anomaly has a higher association with thrombophilia and a thorough hypercoagulable workup should be pursued. There is no consensus on therapy, but anticoagulation, commonly with Enoxaparin, is the mainstay. Endovascular therapies, such as thrombolysis, thrombectomy, and stent placement, are preferable therapies based on patient characteristics.