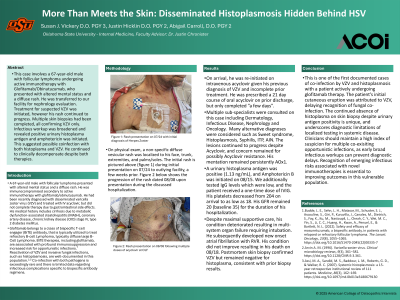
Clinical Scenario or Case: A 67-year-old male with follicular lymphoma presented with altered mental status and a diffuse rash. He was immunocompromised secondary to active immunotherapy with glofitamab/obinutuzumab. He had been recently diagnosed with disseminated varicella zoster virus (VZV) and treated with IV acyclovir, but did not complete therapy due to gastrointestinal side effects. His medical history includes cirrhosis due to metabolic dysfunction-associated steatohepatitis (MASH), coronary artery disease, chronic kidney disease (CKD) stage IV, type 2 diabetes mellitus. On physical exam, a non-specific diffuse vesicular rash was localized to his face, trunk, extremities, and palms/soles. He was re-initiated on intravenous acyclovir given his previous diagnosis of VZV and lack of complete therapy. A urinary histoplasma antigen was positive (1.13 ng/mL), and Amphotericin B was initiated. Despite maximal supportive care, his condition deteriorated, resulting in multi-system organ failure and his demise. Postmortem skin biopsy confirmed VZV but remained negative for histoplasma.
Evidence/Literature Review: Bispecific T-cell engager (BiTE) therapies, including glofitamab, are associated with profound immunosuppression and increased risk for opportunistic infections.¹ Reactivation of VZV and invasive fungal infections, such as histoplasmosis, are well-documented in this population.²˒³ Co-infection with both pathogens is exceedingly rare and there is limited data regarding infectious complications specific to bispecific antibody regimens.
Unique Aspects of Case: This is one of the first documented cases of co-infection by VZV and histoplasmosis with glofitamab therapy. Initial cutaneous eruption was attributed to VZV, delaying recognition of fungal co-infection. This resulted in the patient’s rapid decompensation. The absence of histoplasma on biopsy underscores diagnostic limitations of localized testing in systemic disease.
Recommendations/Conclusions: Clinicians should maintain a high index of suspicion for multiple co-exisiting opportunistic infections, as early broad infectious workups can prevent diagnostic delays. Recognition of emerging infectious risks associated with novel immunotherapies is essential to improving outcomes in this vulnerable population.