Internal Medicine Canyon vista medical center sierra vista, Arizona, United States
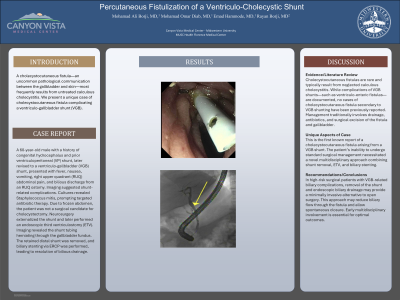
Clinical Scenario or Case: A 60-year-old male with a history of congenital hydrocephalus and prior ventriculoperitoneal (VP) shunt, later revised to a ventriculo-gallbladder (VGB) shunt, presented with fever, nausea, vomiting, right upper quadrant (RUQ) abdominal pain, and bilious discharge from an RUQ ostomy. Imaging suggested shunt-related complications. Cultures revealed Staphylococcus mitis, prompting targeted antibiotic therapy. Due to frozen abdomen, the patient was not a surgical candidate for cholecystectomy. Neurosurgery externalized the shunt and later performed an endoscopic third ventriculostomy (ETV). Imaging revealed the shunt tubing herniating through the gallbladder fundus. The retained distal shunt was removed, and biliary stenting via ERCP was performed, leading to resolution of bilious drainage.
Evidence/Literature Review: Cholecystocutaneous fistulas are rare and typically result from neglected calculous cholecystitis. While complications of VGB shunts—such as ventriculo-enteric fistulas—are documented, no cases of cholecystocutaneous fistula secondary to VGB shunting have been previously reported. Management traditionally involves drainage, antibiotics, and surgical excision of the fistula and gallbladder.
Unique Aspects of Case: This is the first known report of a cholecystocutaneous fistula arising from a VGB shunt. The patient’s inability to undergo standard surgical management necessitated a novel multidisciplinary approach combining shunt removal, ETV, and biliary stenting.
Recommendations/Conclusions: In high-risk surgical patients with VGB-related biliary complications, removal of the shunt and endoscopic biliary drainage may provide a minimally invasive alternative to open surgery. This approach may reduce biliary flow through the fistula and allow spontaneous closure. Early multidisciplinary involvement is essential for optimal outcomes.