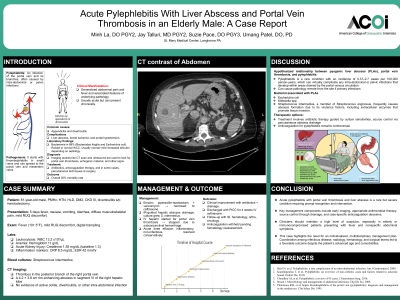
Clinical Scenario or Case: An 81-year-old male with diabetes, chronic kidney disease, and prior hemicolectomy presented with fever, GI symptoms, and diffuse musculoskeletal pain. Labs showed systemic inflammation, and CT revealed a 4.2 × 3.8 cm hepatic abscess and right portal vein thrombosis. Blood and abscess cultures grew Streptococcus intermedius. He was diagnosed with pylephlebitis and treated with IV antibiotics, image-guided abscess drainage, and initially anticoagulated before therapy was halted due to bleeding. He improved and was discharged with outpatient IV antibiotics and multidisciplinary follow-up.
Evidence/Literature Review: Pylephlebitis is a rare but life-threatening complication of intra-abdominal infections, with mortality up to 32%. Diagnosis is often delayed due to nonspecific symptoms. CT imaging is the gold standard; cultures guide antibiotic therapy. While anticoagulation may aid thrombus resolution, bleeding risk—especially in elderly patients—necessitates individualized decisions. S. intermedius, part of the S. anginosus group, is known for its virulence and abscess formation but is an uncommon cause of pylephlebitis.
Unique Aspects of Case: This case is notable for the rare association of S. intermedius with pylephlebitis, the absence of an active intra-abdominal source, and the complex management decisions around anticoagulation in an elderly patient. The patient also developed acute monoarthritis, further complicating the course and requiring multidisciplinary care.
Recommendations/Conclusions: Clinicians should suspect pylephlebitis in elderly patients with fever and vague symptoms, especially with prior abdominal surgery. Early imaging and culture-based antibiotic therapy are critical. Anticoagulation should be carefully weighed. A multidisciplinary approach is key to optimizing outcomes in this high-risk population.