Internal Medicine Rutgers-Jersey City Medical Center Jersey City, New Jersey, United States
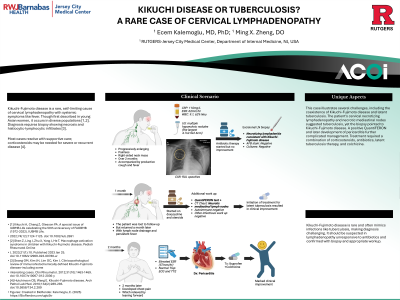
Clinical Scenario or Case: A 28-year-old male presented with a progressively enlarging, painless right-sided neck mass over two months, accompanied by productive cough and fever. Chest X-ray showed a right upper-lobe opacity. Labs showed elevated CRP (110mg/L) and ESR (62mm/hr). Ultrasound demonstrated multiple hypoechoic nodules (the largest 4.7×2.9×2.6cm). Antibiotic therapy was initiated but did not improve symptoms.
Excisional biopsy of the lymph node demonstrated necrotizing lymphadenitis consistent with Kikuchi-Fujimoto disease; acid-fast bacilli stains and cultures were negative. The patient was lost to follow-up but returned a month later with lymph node drainage and persistent fever. He was started on doxycycline and steroids. Additional evaluation revealed a positive QuantiFERON test, and CT imaging demonstrated necrotic mediastinal lymph nodes, while other infectious and autoimmune workups were negative. Initiation of treatment for latent tuberculosis resulted in clinical improvement.
Two months later, the patient developed chest pain which relieved by leaning forward, with elevated ESR (57mm/hr) and normal ECG and echocardiography. Pericarditis was diagnosed and treated with colchicine, leading to marked improvement.
Evidence/Literature Review: Kikuchi-Fujimoto disease is a rare, self-limiting cause of cervical lymphadenopathy with systemic symptoms like fever. Though first described in young Asian women, it occurs in diverse populations[1,2]. Diagnosis requires biopsy showing necrosis and histiocytic-lymphocytic infiltrates[3]. Most cases resolve with supportive care; corticosteroids may be needed for severe or recurrent disease[4].
Unique Aspects of Case: This case illustrates several challenges, including the coexistence of Kikuchi-Fujimoto disease and latent tuberculosis. The patient’s cervical necrotizing lymphadenopathy and necrotic mediastinal nodes suggested tuberculosis, yet biopsy pointed to Kikuchi-Fujimoto disease. A positive QuantiFERON and later development of pericarditis further complicated management. Treatment required a combination of corticosteroids, antibiotics, latent tuberculosis therapy, and colchicine.
Recommendations/Conclusions: Kikuchi-Fujimoto disease is rare and often mimics infections like tuberculosis, making diagnosis challenging. It should be suspected in lymphadenopathy unresponsive to antibiotics and confirmed with biopsy and appropriate workup.